A motor tic is a fast, repetitive series of muscle movements that result in sudden and difficult to control body jolts or sounds. Tics are very common in children from the age of 5 years and it is estimated that 20% of children (1 in 5) experience motor tics at some point. The vast majority of motor tics resolve themselves over time with reassurance for the child without the need for any treatment. Tics and other conditions Tics can occur on their own. In some cases, they are also associated with anxiety, stress or panic disorders. They can be more common in children with Attention Deficit Hyperactivity Disorder (ADHD), Autism Spectrum Disorder (ASD) or Obsessive Compulsive Disorder (OCD).
What are some of the signs of tics?
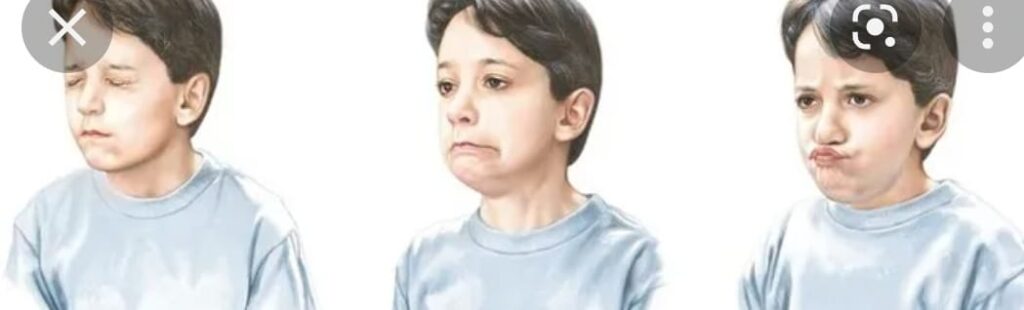
blinking, wrinkling the nose or grimacing
jerking or banging the head
clicking the fingers
touching other people or things
coughing, grunting or sniffing
repeating a sound or phrase – in a small number of cases, this may be something obscene or offensive.
What makes tics worse?
Stress
Tiredness
Boredom
There can be different triggers for each child.
What helps reduce tics?
Distraction and concentrating on other activities which interest your child
Exercise
Better sleep.
How can I help my child?
Here are some suggestions of ways to help manage tics and reduce worry:
Try to ignore your child’s tic and not talk about it too much – drawing attention to it may make it worse
Reassure your child that everything’s OK and there’s no reason for them to feel embarrassed
Ensure that people having regular contact with your child are aware of your child’s tics and explain how best they can respond if one occurs
If your child is finding school difficult, talk to their teacher about ways of dealing with this. For example, it may help if they’re allowed to leave the classroom if their tics are particularly bad.
What are some co-morbidities associated with motor tics
Some co-morbidities are- ADHD, ASD, LD, OCD, Anxiety and Depression
Do Tics need treatment?
Tics are not usually serious and they do not damage the brain. They usually go away on their own. If they are mild and do not cause problems, they might disappear as quickly as they appeared. The treatment modalities are:
Most experts recommend using both medication and behavior therapy to treat ADHD. This is known as a multimodal treatment approach. There are many forms of behavior therapy, but all have a common goal— to change the child’s physical and social environments to help the child improve his behavior. Under this approach, parents, teachers, and other caregivers learn better ways to work with and relate to the child with ADHD. You will learn how to set and enforce rules, help your child understand what he needs to do, use discipline effectively, and encourage good behavior. Your child will learn better ways to control his behavior as a result. You will learn how to be more consistent. Behavior therapy has 3 basic principles.
Tips for helping your child control his behavior Keep your child on a daily schedule. Try to keep the time that your child wakes up, eats, bathes, leaves for school, and goes to sleep the same each day. Cut down on distractions. Loud music, computer games, and TV can be overstimulating to your child. Make it a rule to keep the TV or music off during mealtime and while your child is doing homework. Whenever possible, avoid taking your child to places that may be too stimulating, like busy shopping malls. Organize your house. If your child has specific and logical places to keep his schoolwork, toys, and clothes, he is less likely to lose them. Save a spot near the front door for his school backpack so he can grab it on the way out the door. Reward positive behavior. Offer kind words, hugs, or small prizes for reaching goals in a timely manner or good behavior. Praise and reward your child’s efforts to pay attention. Set small, reachable goals. Aim for slow progress rather than instant results. Be sure that your child understands that he can take small steps toward learning to control himself. Help your child stay “on task.” Use charts and checklists to track progress with homework or chores. Keep instructions brief. Offer frequent, friendly reminders. Limit choices. Help your child learn to make good decisions by giving him only 2 or 3 options at a time. Find activities at which your child can succeed. All children need to experience success to feel good about themselves. Use calm discipline. Use consequences such as time-out, removing the child from the situation or distraction. Sometimes it is best to simply ignore the behavior. Physical punishment, such as spanking or slapping, is not helpful. Discuss your child’s behavior with him when both of you are calm. Principles for behavior therapy Set specific goals. Set clear goals for your child, such as staying focused on homework for a certain time or sharing toys with friends. Provide rewards and consequences. Give your child a specified reward (positive reinforcement) every time she shows the desired behavior. Give your child a consequence (unwanted result or punishment) consistently when she fails to meet a goal. Keep using the rewards and consequences. Using the rewards and consequences consistently for a long time will shape your child’s behavior in a positive way.
Specific Behaviour Therapies are-
1.Positive Reinforcement: E.g Child completes an assignment and is permitted to play on the computer
2.Time Out: E.g Child hits sibling and, as a result, must sit for 5 minutes in the corner of the room
3.Response cost: E.g Child loses free-time privileges for not completing homework
4.Token Economy: E.g Child earns stars or points for completing assignments and loses stars for getting out of seat. The child cashes in the sum of her stars at the end of the week for a prize
Behavior therapy recognizes the limits that having ADHD puts on a child. It focuses on how the important people and places in the child’s life can adapt to encourage good behavior and discourage unwanted behavior. It is different from play therapy or other therapies that focus mainly on the child and his emotions.
How can I help my child control her behavior? As the child’s primary caregivers, parents play a major role in behavior therapy. Parent training is available to help you learn more about ADHD and specific, positive ways to respond to ADHD-type behaviors. This will help your child improve. In many cases parenting classes with other parents will be sufficient, but with more challenging children, individual work with a counselor/coach may be needed. Taking care of yourself also will help your child. Being the parent of a child with ADHD can be tiring and trying. It can test the limits of even the best parents. Parent training and support groups made up of other families who are dealing with ADHD can be a great source of help. Learn stress- management techniques to help you respond calmly to your child. Seek counseling if you feel overwhelmed or hopeless.
What is ADHD? ADHD is one of the most common neurobehavioral disorder affecting children. ADHD is a condition of the brain that makes it difficult for children to control their behavior. It affects 4% to 12% of school-aged children. About 3 times more boys than girls are diagnosed with ADHD.
What are the symptoms of ADHD? ADHD includes 3 groups of behavior symptoms: inattention, hyperactivity, and impulsivity.
Symptoms of attention-deficit hyperactivity disorder (ADHD)
People who have ADHD have difficulty organizing things, listening to instructions, remembering details, and/or controlling their behavior. This can make it difficult to get along with other people at home, at school, or at work.
A person with ADHD who has attention deficit/ difficulty paying attention will have 6 or more of the following symptoms:
Difficulty following instructions
Difficulty keeping attention on work or play activities at school, work, and home
Losing things needed for activities at school, work, and home
Appearing not to listen
Doesn’t pay close attention to details
Seems disorganized
Trouble with tasks that require planning ahead
Forgetting things
Is easily distracted
A person with ADHD who is hyperactive or impulsive will have at least 6 of the following symptoms:
Fidgety
Runs or climbs inappropriately
Can’t play quietly
Blurts out answers
Interrupts people
Can’t stay in seat
Talks too much
Is always on the go
Has trouble waiting his or her turn
Are there different types of ADHD? Not all children with ADHD have all the symptoms. They may have one or more of the symptoms mentioned above. The symptoms usually are classified as the following types of ADHD: Inattentive only – Children with this form of ADHD are not overly active. Because they do not disrupt the classroom or other activities, their symptoms may not be noticed. Among girls with ADHD, this form is most common. Hyperactive/Impulsive—Children with this type of ADHD show both hyperactive and impulsive behavior, but can pay attention. They are the least common group and are frequently younger. Combined Inattentive/Hyperactive/Impulsive—Children with this type of ADHD show a number of symptoms in all 3 dimensions. This is the most common type of ADHD.
How can I tell if my child has ADHD? Remember, it is normal for all children to show some of these symptoms from time to time. Your child may be reacting to stress at school or home. She may be bored or going through a difficult stage of life. It does not mean he/she has ADHD. Sometimes a teacher is the first to notice inattention, hyperactivity, and/or impulsivity and bring these symptoms to the parents’ attention. Perhaps questions from your pediatrician raised the issue. At routine visits, pediatricians often ask questions such as a) How is your child doing in school? b) Are there any problems with learning that you or your child’s teachers have seen? c) Is your child happy in school? d) Is your child having problems completing class work or homework? e) Are you concerned with any behavior problems in school, at home, or when your child is playing with friends? Your answers to these questions may lead to further evaluation for ADHD. If your child has shown symptoms of ADHD on a regular basis for more than 6 months, discuss this with your pediatrician.
Diagnosis It is more difficult to diagnose ADHD in children 5 years of age and younger. This is because children change very rapidly during the preschool years. It is also more difficult to diagnose ADHD once a child becomes a teenager. There is no single test for ADHD. The process requires several steps and involves gathering a lot of information from multiple sources. You, your child, your child’s school, and other caregivers should be involved in assessing your child’s behavior. Children with ADHD show signs of inattention, hyperactivity, and/or impulsivity in specific ways. (See the behaviors listed in Table 1.) Your pediatrician will look at how your child’s behavior compares to that of other children his own age, based on the information reported about your child by you, his teacher, and any other caregivers who spend time with your child, such as coaches or child care workers. To confirm a diagnosis of ADHD, symptoms -Occur in more than one setting, such as home, school, and social situations and cause some impairment -Significantly impair your child’s ability to function in some of the activities of daily life, such as schoolwork, relationships with you and his brothers and/or sisters, and his relationship with friends or in his ability to function in groups such as sports teams -Start before the child reaches 7 years of age (However, these may not be recognized as ADHD symptoms until a child is older.) -Have continued for more than 6 months -In addition to looking at your child’s behavior, your pediatrician will do a physical and neurologic examination. A full medical history will be needed to put your child’s behavior in context and screen for other conditions that may affect his behavior. Your pediatrician also will talk with your child about how he acts and feels. Your pediatrician may refer your child to a pediatric subspecialist if there are concerns in one of the following areas: >Mental retardation >Developmental disorder such as speech problems, motor problems, or a learning disability >Chronic illness being treated with a medication that may interfere with learning >Trouble seeing and/or hearing >History of abuse >Major anxiety or major depression >Severe aggression >Possible seizure disorder >Possible sleep disorder
How can parents help with the diagnosis? As a parent, you will provide crucial information about your child’s behavior and how it affects her life at home, in school, and in other social settings. Your pediatrician will want to know what symptoms your child is showing, how long the symptoms have occurred, and how the behavior affects your child and your family. You may need to fill in checklists or rating scales about your child’s behavior. In addition, sharing your family history can offer important clues about your child’s condition.
How will my child’s school be involved? For an accurate diagnosis, your pediatrician will need to get information about your child directly from your child’s classroom teacher or another school professional. Children at least 5 years of age and older spend many of their waking hours at school. Teachers provide valuable insights. Your child’s teacher may write a report or discuss the following with your pediatrician: -Your child’s behavior in the classroom -Your child’s learning patterns -How long the symptoms have been a problem -How the symptoms are affecting your child’s progress at school -Ways the classroom program is being adapted to help your child -Whether other conditions may be affecting the symptoms In addition, your pediatrician may want to see report cards and samples of your child’s schoolwork.
What causes ADHD? ADHD is one of the most studied conditions of childhood, but ADHD may be caused by a number of things. Research to date has shown -ADHD is a biological disorder. -A lower level of activity in the parts of the brain that control attention and activity level may be associated with ADHD. -ADHD frequently runs in families. Sometimes a parent is diagnosed with ADHD In very rare cases, toxins in the environment may lead to ADHD. Significant head injuries may cause ADHD in some cases. Prematurity increases the risk of developing ADHD. Prenatal exposures, such as alcohol or nicotine from smoking, increase the risk of developing ADHD. There is little evidence that ADHD is caused by: Eating too much sugar/ Food additives/ Allergies/ Immunizations
Treatment Once the diagnosis is confirmed, the outlook for most children who receive treatment for ADHD is very encouraging. There is no specific cure for ADHD, but there are many treatment options available. Each child’s treatment must be tailored to meet his individual needs. In most cases, treatment for ADHD should include A long-term management plan with — Target outcomes for behavior — Follow-up activities — Monitoring Education about ADHD Teamwork among doctors, parents, teachers, caregivers, other health care professionals, and the child Medication Behavior therapy including parent training Individual and family counseling Treatment for ADHD uses the same principles that are used to treat other chronic conditions like asthma or diabetes. Long-term planning is needed because these conditions are not cured. Families must manage them on an ongoing basis. In the case of ADHD, schools and other caregivers must also be involved in managing the condition. Educating the people involved about ADHD is a key part of treating your child. As a parent, you will need to learn about ADHD. Read about the condition and talk to people who understand it. This will help you manage the ways ADHD affects your child and your family on a day-to-day basis. It will also help your child learn to help himself.
Setting target outcomes At the beginning of treatment, your pediatrician should help you set 3 to 6 target outcomes (goals) for your child’s behavior. These target outcomes will guide the treatment plan. Your child’s target outcomes should focus on helping her function as well as possible at home, at school, and in your community. You need to identify what behaviors are most preventing your child from success. The following are examples of target outcomes: • Improved relationships with parents, siblings, teachers, and friends (eg, fewer arguments with brothers or sisters or being invited more frequently to friends’ houses or parties) • Better schoolwork (eg, completing class work or homework assignments) • More independence in self-care or homework (eg, getting ready for school in the morning without supervision) 6 • Improved self-esteem (eg, increase in feeling that she can get her work done) • Fewer disruptive behaviors The target outcomes should be Realistic, Something your child will be able to do, and behaviors that you can observe and count.
Medication For most children, stimulant medications are a safe and effective way to relieve ADHD symptoms. As glasses help people focus their eyes to see, these medications help children with ADHD focus their thoughts better and ignore distractions. This makes them more able to pay attention and control their behavior. Stimulants may be used alone or combined with behavior therapy. Studies show that about 80% of children with ADHD who are treated with stimulants improve a great deal once the right medication and dose are determined. Different types of stimulants are available, in short-acting (immediate- release), intermediate-acting, and extended-release forms. (See Table 2.) Immediate-release forms usually are taken every 4 hours, when the medication is needed. They are the cheapest of the medications. Intermediate-acting and extended-release medications usually are taken once in the morning. Children who use extended-release forms of stimulants can avoid taking medication at school or after school. It is important not to chew or crush extended-release capsules or tablets. However, extended-release capsules that are made up of beads can be opened and sprinkled on food for children who have difficulties swallowing tablets or capsules. Which medication is best for my child? It may take some time to find the best medication, dosage, and schedule for your child. Your child may need to try different types of stimulants or other medication. Some children respond to one type of stimulant but not another. The amount of medication (dosage) that your child needs also may need to be adjusted. The dosage is not based solely on his weight. Your pediatrician will vary the dosage over time to get the best results and control possible side effects. The medication schedule also may be adjusted depending on the target outcome. For example, if the goal is to get relief from symptoms mostly at school, your child may take the medication only on school days. It is important for your child to have regular medical check-ups to monitor how well the medication is working and check for possible side effects.
What side effects can stimulants cause? Side effects occur sometimes. These tend to happen early in treatment and are usually mild and short-lived, but in rare cases can be prolonged or more severe. The most common side effects include Decreased appetite/weight loss Sleep problems Social withdrawal Some less common side effects include Rebound effect (increased activity or a bad mood as the medication wears off) Transient tics Very rare side effects include Significant increase in blood pressure or heart rate Growth delay Bizarre behaviors Most side effects can be relieved by Changing the medication dosage Adjusting the schedule of medication Using a different stimulant or atomoxetine Close contact with your pediatrician is required until you find the best medication and dose for your child. After that, periodic monitoring by your doctor is important to maintain the best effects. Stimulants and atomoxetine may not be an option for children who are taking certain other medications or who have some medical conditions such as congenital heart disease.
How can my child’s school help? Your child’s school is a key partner in providing effective behavior therapy for your child. In fact, these principles work well in the classroom for most students. Classroom management techniques may include Keeping a set routine and schedule for activities Using a system of clear rewards and consequences, such as a point system or token economy Sending daily or weekly report cards or behavior charts to parents to inform them about the child’s progress Seating the child near the teacher Using small groups for activities Encouraging students to pause a moment before answering questions Keeping assignments short or breaking them into sections Close supervision with frequent, positive cues to stay on task Your child’s school should work with you and your pediatrician to develop strategies to assist your child in the classroom. It is important to remember that once diagnosed and treated, children with ADHD are more likely to achieve their goals in school. Keeping the treatment plan on track Ongoing monitoring of your child’s behavior and medications is required to find out if the treatment plan is working. Office visits, phone conversations, behavior checklists, written reports from teachers, and behavior report cards are common tools for following the child’s progress. Treatment plans for ADHD usually require long-term efforts on the part of families and schools. Medication schedules may be complex. Behavior therapies require education and patience. Sometimes it can be hard for everyone to stick with it. Your efforts play an important part in building a healthy future for your child. Ask your pediatrician to help you find ways to keep your child’s treatment plan on track. Unproven treatments You may have heard media reports or seen advertisements for “miracle cures” for ADHD. Carefully research any such claims. Consider whether the source of the information is valid. At this time, there is no scientifically proven cure for this condition. The following methods have not been proven to work in scientific studies: • Megavitamins and mineral supplements • Anti–motion-sickness medication (to treat the inner ear) • Treatment for candida yeast infection • EEG biofeedback (training to increase brain-wave activity) • Applied kinesiology (realigning bones in the skull) • Reducing sugar consumption • Optometric vision training (asserts that faulty eye movement and sensitivities cause the behavior problems) Always tell your pediatrician about any alternative therapies, supplements, or medications that your child is using. These may interact with prescribed medications and harm your child.
Will there be a cure for ADHD soon? While there are no signs of a cure at this time, research is ongoing to learn more about the role of the brain in ADHD and the best ways to treat the disorder. Additional research is looking at the long-term outcomes for people with ADHD.
Will my child outgrow ADHD? ADHD continues into adulthood in most cases. However, by developing their strengths, structuring their environments, and using medication when needed, adults with ADHD can lead very productive lives. In some careers, having a high-energy behavior pattern can be an asset.
Infantile spasms are a type of seizures that tend to affect children under the age of 2 years. In this, children have tightening and jerky movements of limbs and body. These usually occur in clusters. Clusters of spasms usually occur upon awakening but can happen at any time of the day.
What is West Syndrome?
West syndrome is a clinical condition characterised by the combination of o Infantile spasms o Abnormal EEG showing chaotic pattern called Hypsarrhythmia o Delayed development or loss of acquired milestones.
Why is it called ‘West’ Syndrome?
West Syndrome is named after the English surgeon Dr.William James West, who published the first description of infantile spasms in 1841, having witnessed the disease in his own son, James E West. He named the seizures “Salaam Tics” at the time.
How do I recognise infantile spasms?
Infantile spasms manifest in different forms. These usually consist of a brief interruption of behaviour, with lifting and extension of the arms and bending forward at the waist. This may be accompanied by a rapid and forceful drop of the head. The individual spasms last a few seconds. Spasms often occur in clusters and the child may have several of them in a row, although singles spasms are possible. After the first spasm, there is a pause and then another spasm follows. Each cluster typically lasts a few minutes. After individual spasms, children often cry. They usually occur as child wakes up from sleep.
What is the cause of infantile spasms?
Almost any brain abnormality or injury to the brain has the potential to cause infantile spasms. Examples include brain malformations, brain infections, problems at birth and neonatal period such as delayed cry leading to lack of oxygen or low sugar levels. About one-tenth of children with infantile spasms may not have an identifiable cause despite detailed evaluation.
What is the outcome of West syndrome?
The outcome of West syndrome is highly variable; however, it is generally difficult to treat and commonly associated with developmental delay and future epilepsy. Early diagnosis and treatment of West syndrome helps in better seizure control and improved developmental outcome.
How is West Syndrome diagnosed?
The main modality of diagnosis of West Syndrome is an electroencephalogram (EEG), on which a chaotic pattern of brain waves called as hypsarrhythmia is the characteristic abnormality noted in West Syndrome. Apart from this, other investigations like MRI of the brain are done to find out the underlying cause.
How is West Syndrome treated?
A number of treatment modalities are available. The most effective drug therapies include ACTH and steroids and a drug called vigabatrin. Other anti-seizure medications are also used, though these are less effective. These include valproate, zonisamide, topiramate , clonazepam and clobazam. A one-week trial of pyridoxine is usually given at the beginning in all patients.
What are the side effects of steroids?
High dose steroids used for treatment of West Syndrome. Prolonged steroid therapy can have side effects like
· Irritability
· Increased appetite
· Weight gain
· High blood pressure
· High blood sugar levels
· Increased risk of infections
There are however transient and improve when steroid therapy is stopped.
What precautions need to be undertaken while the child is on steroids?
Any vaccines should be given to the child after consultation with the treating doctor. Children on high dose steroids for more than 2 weeks must not be given live vaccines like oral polio vaccine, measles, mumps, varicella vaccines until at least 1 month of stopping the steroids. These children are more prone to infections; hence parents should report to the hospital if the child has fever.
What are the side effects of other drugs?
Vigabatrin can cause visual disturbances when used for long duration. Valproate can cause affect liver and pancreas in high doses.
Is there any treatment apart from drugs?
In children who do not respond to anti-seizure or hormonal therapies, other modalities like surgery (to remove seizure-generating parts of the brain) and ketogenic diet may be tried.
What is ketogenic diet?
Ketogenic diet is a specialized very-high fat diet used in treating many types of epilepsy. It involves strict adherence to a diet plan and required monitoring by an experienced neurologist.
How long is the treatment continued?
Steroids are usually given for about 2 weeks followed by slowly tapering the dose and stopping. Vigabatrin is usually continued for 6 months. Other anti-seizure medications are usually continued for a couple of years till seizure control is attained.
Learning disorder includes a heterogeneous group of disorders manifested by significant difficulties in the acquisition and use of reading (dyslexia), writing (dysgraphia), or mathematical (dyscalculia) abilities despite intact senses, normal intelligence, proper motivation, and adequate socio-cultural opportunity.
Having a learning disorder means that a child has difficulty in one or more areas of learning, even when overall intelligence or motivation is not affected. Symptoms of learning disorders are:
-Difficulty telling right from left
-Reversing letters, words, or numbers, after first or second grade
-Difficulties recognizing patterns or sorting items by size or shape
-Difficulty understanding and following instructions or staying organized
-Difficulty remembering what was just said or what was just read
-Lacking coordination when moving around
-Difficulty doing tasks with the hands, like writing, cutting, or drawing
-Difficulty understanding the concept of time
According to DSM-5, the diagnosis of a specific learning disorder includes the following symptoms:
1. During formal years at school, persistent difficulties in reading, writing, arithmetic, or mathematical reasoning skills can be identified by symptoms such as inaccurate or slow and effortful reading, poor written expression, difficulties remembering number facts, or inaccurate mathematical reasoning.
2. Current academic abilities must fall far short of the typical range of scores on linguistically and culturally relevant reading, writing, and arithmetic examinations. As a result, a dyslexic person must read with significant effort and not in the same way that a regular reader does.
3. Learning problems originate in the early years of schooling.
4. The individual’s difficulties must markedly impair academic success, occupational performance, or daily activities, and they must not be explained by developmental, neurological, sensory (vision or hearing), or motor disorders.
Examples of learning disorders include
1.Dyslexia – difficulty with reading
E.g
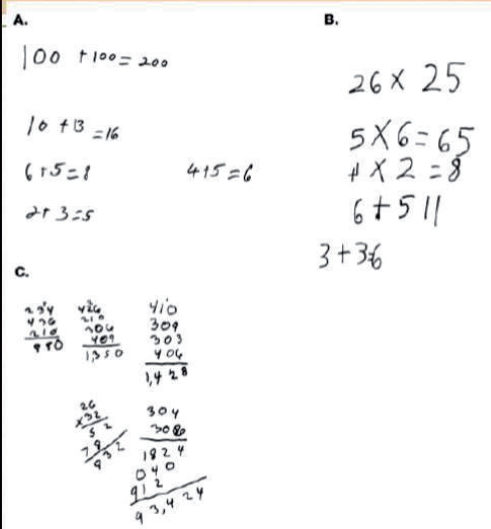
2.Dyscalculia – difficulty with math
E.g
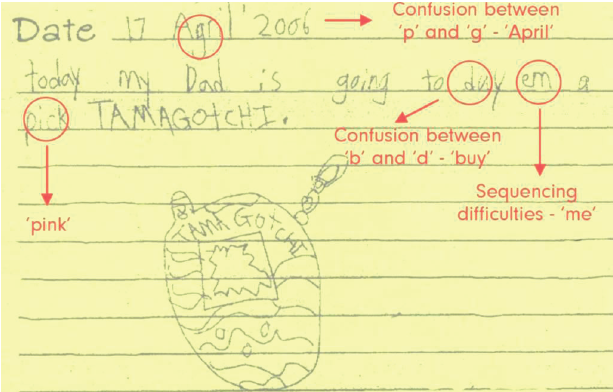
3.Dysgraphia – difficulty with writing
E.g
4.Language processing disorder
5.Nonverbal learning disabilities
6.Visual perceptual disabilities
Language Processing Disorder (LPD) relates to the difficulties in processing of expressive language and/or receptive language. Non-verbal learning disability refers to problems in understanding nonverbal cues like facial expressions or body language. Visual processing disorder includes trouble drawing or copying, inability to detect differences in shapes or letters, and letter reversals.
The major causes of learning disabilities are inherited cause, genetic cause, neurobiological or brain injury, co-morbid disorders, environmental factors. They recognize autism spectrum disorder (ASD) and attention deficit hyperactivity disorder (ADHD) as related disorders that impact learning, though not specific learning disorders.
Learning disorders can also be present with emotional or behavioral disorders, such as attention-deficit/hyperactivity disorder (ADHD), or anxiety. The combination of problems can make it particularly hard for a child to succeed in school. Properly diagnosing each disorder is crucial, so that the child can get the right kind of help for each.
Treatment
They often need extra help and instruction that are specialized for them. Having a learning disorder can qualify a child for special education services in school. SLD could cause complications if not remedied earlier. Intense and focused instruction may in fact alter the brain activation profiles observed in children with SLD. Hence there is a need to advocate for intense and focused instruction in each of the affected academic domains. There are Accomodation and Modification based therapies.